The specific device-aided therapy chosen must be customized to a patient’s particular symptoms. Some symptoms only improve with a specific device-aided therapy. For example, troublesome tremor, despite aggressive oral treatment, generally responds only to DBS or FUS.
There may be advantages to starting with the less invasive and more easily reversible device-aided therapies. This may allow a patient to function well without exposure to more severe side effects. Patients may always try additional more invasive device-aided therapies in the future, if necessary.
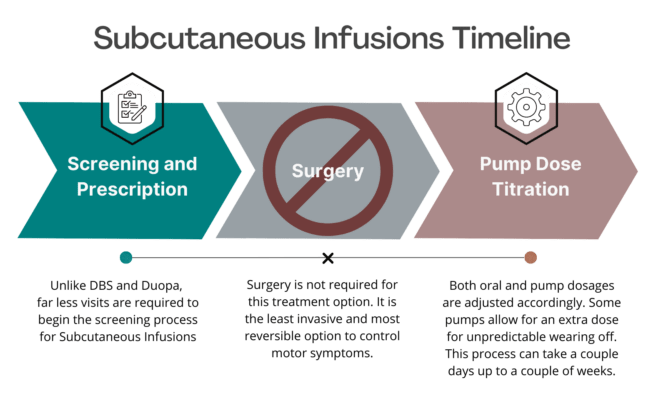
Introducing the potential for an upcoming Subcutaneous Infusion Pump designed to provide a steady dose of apomorphine directly under the skin to reduce OFF episodes and troublesome dyskinesia in Parkinson’s disease. Unlike other devices, this option is minimally invasive, discreet, and easily concealed, and does NOT require surgery or hospitalization.
Patients have the flexibility to remove the pump whenever they choose (i.e. in the shower) offering a level of convenience and control over their treatment regimen. This therapy is both easy to start and stop, allowing patients to explore its benefits without the commitment of irreversible surgery, making it a significant alternative to considering Deep Brain Stimulation (DBS).
Clinical studies determined that this Infusion Pump reduced OFF time by an average of 3 hours with a similar increase in good ON time without troublesome dyskinesia. Once approval is gained, this pump will be the first and only continuous infusion device available for PD.
Subcutaneous infusion therapy is not a cure for Parkinson’s Disease and it does not slow PD progression. It generally does not help any Parkinson’s disease symptoms that do not improve with your best medication “on” time.
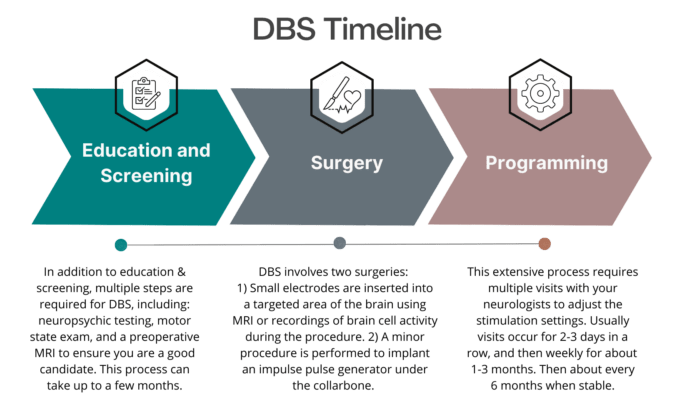
Deep brain stimulation (DBS) is a treatment for neurological conditions such as Parkinson’s disease, essential tremor, and epilepsy. DBS was first approved for the treatment of PD in 1997 and involves the surgical implantation of an electrode in the brain in an area important for the control of movement, specifically in a region called the globus pallidus internus (GPi) or the subthalamic nucleus (STN). Wires passing through the neck connect the electrode to a stimulator in the chest. The stimulator is a small pacemaker-like device that delivers a controlled electronic pulse to the brain.
Two regions in the brain may be chosen for electrode placement: the subthalamic nucleus (STN) or the globus pallidus internus (GPI). The area chosen depends on a patient’s symptoms. Both areas are very effective for a patient’s tremor and slowness. A clinician may be more likely to choose the STN if a patient experiences many adverse effects from carbidopa/levodopa such as excess dyskinesia. Stimulation of the STN often allows for greater medication reduction than stimulation of the GPi. There is some data to suggest that stimulation of the GPi leads to fewer problems with language and cognition. Many ongoing studies will help refine target choices for individual patients.

Focused Ultrasound therapy has emerged as a promising non-invasive treatment option for Parkinson’s disease, offering hope to patients grappling with its debilitating symptoms. By utilizing precisely targeted ultrasound waves to target areas of the brain, this approach aims to alleviate motor symptoms such as tremors, rigidity, and bradykinesia.
Unlike traditional surgical interventions, Focused Ultrasound therapy doesn’t involve incisions or anesthesia, minimizing the risk of complications and reducing recovery time. With ongoing research and clinical trials showing promising results in symptom management and improving quality of life, Focused Ultrasound therapy presents a potential breakthrough in the treatment landscape for Parkinson’s disease.

Duopa therapy is a form of carbidopa/levodopa delivered in gel form (called enteral suspension) directly to where the medication is absorbed in the small intestine. Before Duopa may be started, a patient needs to get a minor surgery to make a small hole, called a stoma, in the stomach wall to place a tube in the intestine. A pump then delivers the gel form of levodopa directly to the intestine through this tube. Duopa is the same active ingredient as the oral carbidopa/levodopa. It is helpful to improve absorption of the medication and reduce “off” time by delivering the drug directly to the small intestine.
There are 3 components to Duopa: 1. PEG-J Tube: Delivers medication into the body, directly through the intestine. To clean the tubing and prevent blockages, it should be flushed with a syringe before and after every pump use. Routine care will vary depending on the type of PEG-J tubing used. 2. Cassette: Contains the gel Carbidopa/Levodopa (2,000mg). A new cassette must be used daily, and discard any leftover medication. One cassette can be used up to 16 hrs. a day. Some patients may need up to 2 cassettes per day. Cassettes must be stored in the refrigerator. 3. Duopa Pump: The pump is programmed for individual needs. Pump settings include 3 doses: A large morning dose to get to an “on” state. Then switches to a lower continuous dose each hour to maintain the “on” state. Lastly, an extra dose is prepared as needed for unexpected “off” time.
Once your neurologist determines that Duopa therapy is appropriate for you, you will meet with a GI specialist to discuss the PEG-J tube procedure. If you have had certain surgeries on your abdomen, such as bariatric surgery or removal of part of your intestines, then you may not be eligible to receive Duopa.
Duopa allows for continuous infusion of levodopa for up to 16 hours per day. Your continuous rate settings will provide most of your daily medication, and you may give yourself extra doses with the pump if needed. Generally, symptoms do not improve beyond what a patient considers good “on” time before Duopa therapy.
Some people choose to continue their other Parkinson’s medications (such as dopamine agonists or amantadine), although you often can stop these medications once you have the pump. At night, you can expect to take your oral medication as normal.
Duopa is not a cure for Parkinson’s Disease and it does not slow PD progression. Duopa generally does not help any Parkinson’s disease symptoms that do not improve with your best medication “on” time.
There was a problem reporting this post.
Please confirm you want to block this member.
You will no longer be able to:
Please note: This action will also remove this member from your connections and send a report to the site admin. Please allow a few minutes for this process to complete.
{kind=link}
{kind=link}
{kind=link}
{kind=link}